1940 阅读 2020-02-11 14:22:23 上传
The Effect of Hearing Loss on the Vocal Features of Children
Fatemeh Kasbi1 ; Ali Sadollahi1 ; Jalal Bakhtiyari1 ; Raheb Ghorbani2 ; Marziyeh Maddah3 ; Maryam Mokhlesin1,*
1Neuromuscular Rehabilitation Research Center, Rehabilitation College, Semnan University of Medical Sciences, Semnan, IR Iran
2Research Center for Social Factors Effective on Health, Semnan University of Medical Sciences, Semnan, IR Iran
3Rehabilitation College, Semnan University of Medical Sciences, Semnan, IR Iran
*Corresponding author: Maryam Mokhlesin, Neuromuscular Rehabilitation Research Center, Rehabilitation College, Semnan University of Medical Sciences, Semnan, IR Iran. Tel: +98-2333654180, Fax: +98-2333654209, E-mail:m_mokhlessin@yahoo.com
Received: March 13, 2013; Revised: June 29, 2013; Accepted: July 13, 2013
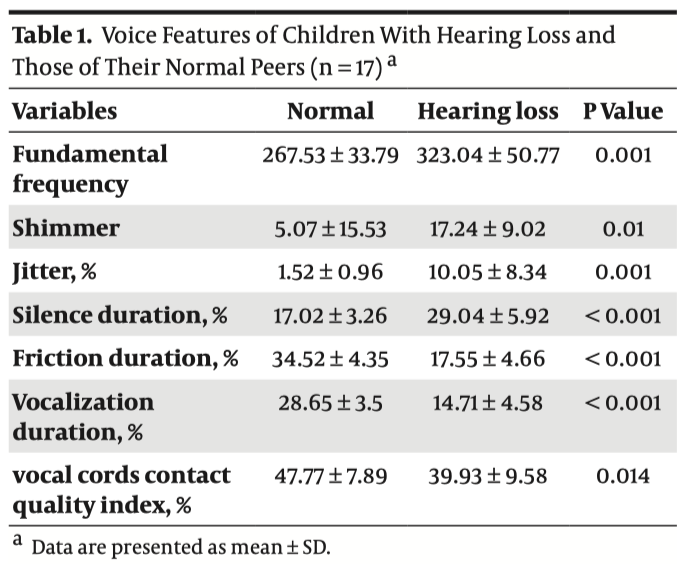
Background: It is difficult to determine the effect of hearing loss pathologic factors on the vocal features rather than other parts of speech, due to the complication of nature of voice, its vast range of changes, and lack of necessary standards and criteria. Objectives: The current study aimed to evaluate the effect of hearing loss on acoustic properties of voice through acoustic analysis of some vocal parameters in two groups of children with moderately severe or deep hearing loss, and normal children of the same age and gender. Patients and Methods: The current study was a comparative cross-sectional descriptive analysis of primary school students with severe to deep hearing loss disorder (n = 17) and normal students (n = 17) of the same age and gender. Data were collected using Speech Studio software and Laryngograph apparatus. To compare parameters between the two groups T-test (P < 0.05) was performed. Results: The mean of fundamental frequency for the hearing loss children and the control group were 323.04 Hz and 267.53 Hz, jitter 10.05% and 1.52%, shimmer 17.24 and 5.07, silence duration 29.40% and 17.02%, friction duration 17.55% and 34.52% and vocalization duration 14.71% and 28.65%, and vocal cords contact quality index 39.93% and 47.77%, respectively. Conclusions: Significant difference in the fundamental frequency, jitter, shimmer, silence duration, friction duration, vocalization duration, and vocal cords contact quality index between the two groups was observed (P < 0.01). Keywords: Hearing Loss; Friction; Voice, Acoustic Parameters; Electrolaryngograph |
1. Background
Normal voice has proper quality, pitch, loudness, and flexibility (1). Hearing loss is an important factor which affects the aforementioned parameters, makes them out of normal, and causes voice disorders (2). Phonation Monitoring is through three sources: 1. kinesthetic feedback, 2. tactile feedback, and 3. auditory feedback. Auditory feedback is constantly controlling the coarse speech features such as: pitch, quality and intensity, and also breathiness voice (2-8). Against possessing the healthy biological features to produce voice (respiratory system, laryngeal cavity, speech production and resonator organs) hearing loss people have problems with vocalization and speech production (9-13). The result of auditory feedback deprivation is that the patient cannot control his vocal performance automatically which results in vocalization disorders and lack of voice quality; in a way that patients with such disorders usually have breathy, rough, weak, unvoiced, and strident voice which lacks melody and dynamics (1, 12-18). Hence, these people usually use their kinesthetic feedback to increase their vocal sense or sustain their ideal speech products. Using kinesthetic feedback causes more tension, and increases muscular and vocal pressure (3, 9, 10, 19). Disability in sustaining fine and stable tension in vocal cords causes these people not to be able to produce more than one tone and adapt their voice with different frequencies and dynamics, or change it constantly and continuously (20). Studies on the effects of hearing loss on voice, with emphasis on specific vocal features in different age groups, started in the recent decades (3, 6-8, 10-17, 19-32), and to analyze vocal features different data collection tools were applied. Also, some studies evaluated the speech and vocal features in people who have done cochlear implant, before and after the surgery.
Matrony studied 22 children with moderately severe hearing loss and measured their fundamental frequency in monosyllabic words through analytical- conceptive method. He showed that variations. Giusti et al. compared variability of f0 and fundamental frequency in children with sensorineural hearing loss (from intense to deep) and normal children using Dr. Speech software. They reported that the fundamental frequency and its variability were higher in children with hearing loss than normal children (16). In a descriptive analytical survey, Girgin studied speech samples of 35 high school Turkish girls with congenital in average fundamental frequency level and within its band range are either very high or very low (21). Stratton evaluated sentence intonation in 12 children with severe to deep hearing loss disorders through analytical-conceptive method. He found that they cannot increase their control over the fundamental frequency to stress and sustain fundamental frequency increases in the end of the interrogative sentences (22). Monsen et al. also reported that some patients with hearing impaired have periods with allophone, voice failure and symptoms of irregularity in fundamental frequency and voice intensity; and they have no control over the tension of vocal cords and the pressure under glottis (23). sensorineural hearing loss. He showed that the pitch range in these patients was more limited and their pitch level was higher than those of their normal classmates (27). Leiska who evaluated the voice of 35 patients with profound congenital hearing loss by VFMs reported that their fundamental frequency was higher than those of their normal peers (3). Hocevar-Boltezar et al. longitudinally evaluated vocal features of two groups of children with pre-lingual hearing loss who did cochlear implant before and after age of four, before and 6, 12, and 24 months after the surgery using Multi Dimension Voice Program and Key Elemetric USA method. They showed that children who did the surgery before the age of four, six months after surgery experienced jitter and shimmer reduction and also showed NHR reduction within 12 months after surgery, while their f 0 increased. On the other hand, in children who did cochlear implant after the age of four, f 0 , and jitter and shimmer reduced within six months and 12 months after surgery respectively, and no change in NHR was observed (29).
Bolfan-Stosic et al. evaluated jitter, shimmer and NHR of children with slight upward hearing loss using high – quality sound level meter, Brucl&Kjaer real-time. They reported that jitter and shimmer in hearing loss children were significantly higher and their NHR was lower than those of the normal children (28). In the study of Kent and Ball cited by Cowei vocal features of a child with congenital deep hearing loss were evaluated using electro-laryngograph apparatus. Based on their study, the friction and vocalization durations in the child were significantly lower than those of a normal child and the vocal cords contact quality index was out of range in comparison with that of a normal child (32). Dehqan et al. evaluated the speech samples of boys with deep hearing loss using Dr. Speech software. The mean of f0, jitter, and shimmer in these patients was higher, and their HNR was lower than those of the normal boys (33). Since language, culture , and accent of each region affect the acoustic features, and also considering the point that there were insufficient data regarding the effects of hearing loss on the voice of the patients speaking the Persian language, the current study aimed to evaluate the effects of hearing loss on children`s voice through acoustic analysis of vocal parameters in two groups of hearing loss and normal children with the mean age of 10.58 years and the same gender by Laryngograph apparatus and Speech Studio software. Results of the current study also provided information about the effect of hearing on the voice of people.
2. Objectives
The obtained results can provide viewpoints regarding the strategies of therapeutic programs and their evaluation in the speech therapy of these children.
3. Patients and Methods
The current study was a comparative cross-sectional descriptive analysis performed on 17 children with two-sided sensorineural hearing loss with the mean age of 10.6 years (12.6 to 7.4 years) and moderately severe hearing loss (61-75 DB) to deep hearing loss (+ 96 DB) with hearing loss background before language learning age using the available sampling method. Subjects were selected from Semnan School for the Deaf and 17 children of the same age and gender were also selected by random selection method from public schools of Semnan city, Iran as the control group (mean age of 10.2 years, 7.1 to 12). Exclusion criteria were syndromes, neuromuscular disorders (dysarthria), visual impairments (except for refractive errors) and mental retardation. Level of education for the children with hearing loss and normal children were primary school and primary/guidance school, respectively. Regarding the gender, there were eight boys and nine girls in each group.
3.1. Data Collection Tool
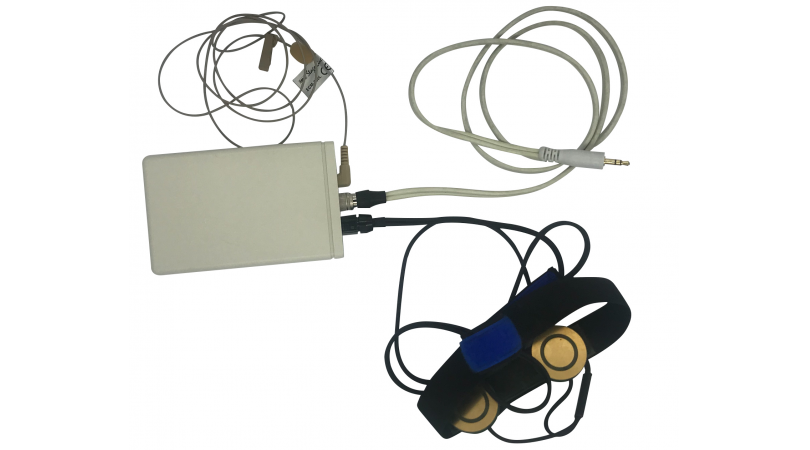
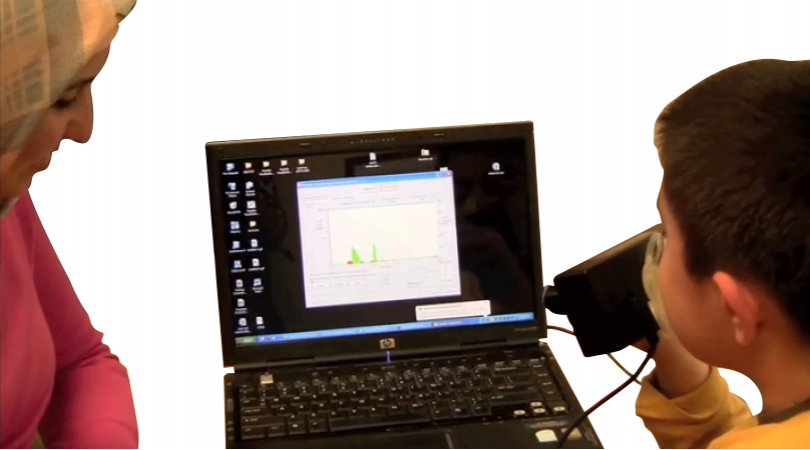
To collect data for the current study, questionnaires, Speech Studio software and Laryngograph apparatus were used. Questionnaires were designed for the two groups, normal children and children with hearing loss, separately.
1) Questionnaire for the children with hearing loss contained two parts. The first part included demographic data such as: age, gender, duration of hearing loss onset, duration of using hearing aids, and level of hearing loss. And the second part included exclusion criteria such as syndromes, dysarthria, visual impairments (except for refractive errors) and mental retardation. Based on the students’ records, if a student had one of these items he was excluded from the survey.
2) Questionnaire for normal children also contained two parts. The first part included demographic data such as: age and gender. The second part was the same as that of the first questionnaire.
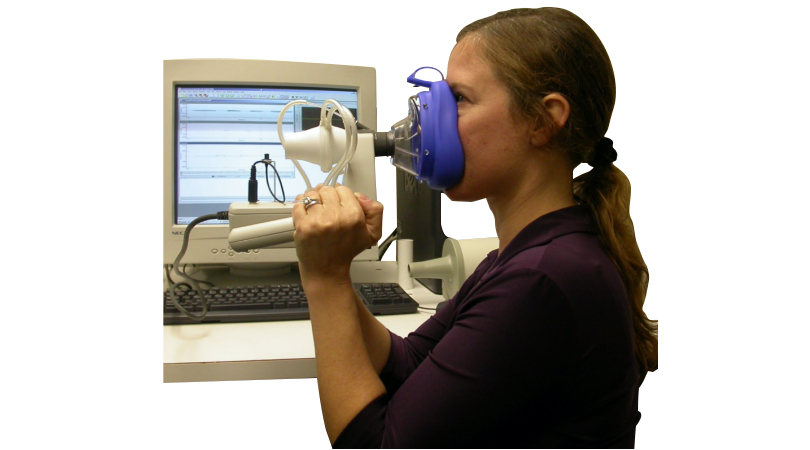
Subjects were referred to the clinical laboratory of the Speech Therapy Clinic. Electrodes of Laryngograph apparatus were attached on thyroid joints of the children and microphone was adjusted 10 cm from the mouth of the subjects. Tests were performed in a soundproof room, and for the children with hearing loss the hearing aid was removed before the test. Subjects were requested to produce the sound/a/ for 10 seconds, and since some of them could not count more than 10 were requested to count from one to ten twice.
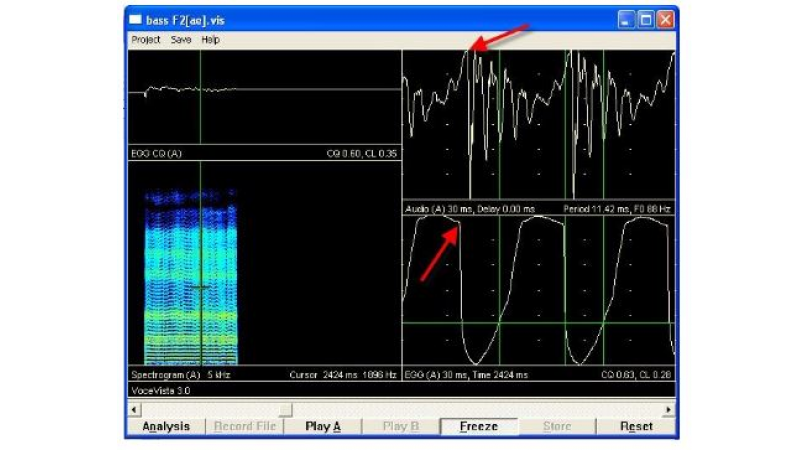
Before recording the voice sample, subjects practiced producing the sound or the counting task at least three times to prevent any mistakes during recording. Also, since vocalization initiation is associated with some irregularities in vibration of vocal cords, the first three seconds of the recordings were ignored. The samples recorded from both groups were analyzed by the aforementioned tools, and the data collected from fundamental frequency, frequency turbulence, voice intensity, silence duration, friction duration, vocalization duration, and vocal cords contact quality index were analyzed using SPSS v. 11.5. To evaluate normality of data, KolmogorovSmirnov test was performed, and to compare the mean data of each parameter between the groups, T-student test was used, at the significance level of 5%.
4. Results
Results of the current study showed significant difference in the mean of fundamental frequency, jitter, and voice intensity, silence duration, friction duration, vocalization duration, and vocal cords contact quality index between both groups (P < 0.05); in a way that the mean of fundamental frequency, jitter and loudness and also silence duration of children with hearing loss was more than those of normal children, and vocalization duration, and vocal cords contact quality index of children with hearing loss was lower than those of the normal children (Table 1).
5. Discussion
Based on the results of the current study, the mean of fundamental frequency of children with hearing loss was significantly higher than that of their peers (P = 0.0001). These results were compatible with those of Dehqan and Giusti who used Dr. Speech software (16, 32), Leiska who used VFMs apparatus (3), and Girgin et al. who performed conceptual analysis (27). Also, the results of the current study were similar to those of Megan et al. on adults with hearing loss before cochlear implant, using CSL, and Nasometer (30), but were incompatible with those of Weath-erley et al. who studied the elderly with hearing loss (25). High fundamental frequency in people with hearing loss may result from high pressure under the glottis; to control and measure the voice, these people try to increase their vocal sense (7). Regarding the incompatibility of the current results with those of Weatherley et al. based on the findings of Waldstein, incidence of hearing loss after learning the language has negligible or no effect on the speech, since speech skills have been developed completely and production mechanisms have been automatized; therefore, there is no need for auditory feedback (8). Maegan, Dophi, Cocker, Sergint and Ross also believed that the acquired hearing loss in adults usually does not affect their speech and probably increases their loudness (30, 34).
Also, the mean of jitter and shimmer in the children with hearing loss were 10.05 and 17.24 respectively which were significantly higher (P < 0.01) in comparison with the results of the control group (1.52 and 5.07 respectively). Results of the other studies also confirm those of the current study (6-8, 31, 33). Increase in jitter and shimmer may result from low control over respiratory protection and the nerves of laryngeal muscles of people with hearing loss which cause large outflow of air from glottis and irregular vibration of the vocal cords (28, 35-37).
Silence duration, friction, vocalization, and vocal cords contact quality index were studied in the current study and the results showed that silence duration in children with hearing loss was longer than that of their normal peers (29.4% compared to 17.02%), (P < 0.001); but friction and vocalization durations and vocal cords contact quality index in children with hearing loss were lower than those of their normal peers (17.55%, 14.71% and 39.93% compared to 34.52%, 28.65% and 47.77%), (P < 0.001) which is compatible with the results of Kent and Ball cited by Kent et al. (32).
Vocal cords contact quality index is an index to determine the quality of voice. In people with hearing damage, disorders in the quality of voice and scrambled voice may result from tonus and stiffness in breathing, vocalization, and speech products procedures, due to failure in feedback mechanisms, to control the voice and speech which results in vocal features damage. It may cause Breathiness voice which is diagnosed by breathy voice associated with noise and results in HNR reduction (28, 38-40). In the current study, mean fundamental frequency, jitter, shimmer, and silence duration of children with hearing loss were higher than those of normal children; and in contrast, vocal cords contact quality index, friction and vocalization durations in children with hearing loss were lower than those of their normal peers and the difference was significant (P < 0.0001). Since the current study was conducted on a small population of children with moderately severe or deep hearing loss it cannot be generalized to the total community understudy; therefore, it can be a topic for further studies and to obtain more generalized results, separation of different ranges of hearing loss in different age ranges is recommended; these results can be applied in further therapeutic programs and provide proper feedback during treatment and also help in the production of new hearing aids.
Acknowledgements
The authors thank the officials of Education Bureau in Semnan for their help and also Ms Mahboubeh Namjou and Ms Maryam Rafati who have contributed in collecting the data.
Authors’ Contributions
It is to be mentioned that Ms F. Kasbi in presenting, compiling and performing the proposal, Mr A. Sadollahi, Mr J. Bakhtiyari and Ms M. Maddah and Ms M. Mokhlesin in writing and administering it, Mr R. Ghorbani in analyzing the data and also Ms M Mokhlesin in writing this article have contributed.
References
1. Boone DR, McFarlane SC, Von Berg SL. The voice and voice therapy.Boston: Pearson/Allyn & Bacon; 2005.
2. Johnson JP, Moulton RD. Nature and treatment of articulation disorders.: Thomas; 1980.
3. Lejska M. Voice field measurements--a new method of exami-nation: the influence of hearing on the human voice. J Voice. 2004;18(2):209–15. 4. Yates AJ. Delayed auditory feedback. Psychol Bull. 1963;60(3):213.
5. Siegel GM, Pick HL, Jr. Auditory feedback in the regulation of voice. J Acoust Soc Am. 1974;56(5):1618–24.
6. E. Lman JL . Effects of frequency-shifted feedback on the pitch of vocal productions. J Acoust Soc Am. 1981;70(1):45–50.
7. Zimmermann G, Rettaliata P. Articulatory patterns of an adventi-tiously deaf speaker: implications for the role of auditory information in speech production. J Speech Hear Res. 1981;24(2):169–78.
8. Waldstein RS. Effects of postlingual deafness on speech production: implications for the role of auditory feedback. J Acoust Soc Am. 1990;88(5):2099–114.
9. Lejska M. The Verbal Communicational Disorders and Phoniatry.Brno: Czech Republic paido; 2002.
10. Monsen RB. The oral speech intelligibility of hearing-impaired talkers. Journal of Speech Hear Disord. 1983;48(3):286–96.
11. Monsen RB. Acoustic qualities of phonation in young hearing-impaired children. J Speech Hear Res. 1979;22(2):270–88.
12. Calvert DR. Deaf voice quality-a preliminary investigation. Volta Rev. 1962;64(7):402–3.
13. Lejska M. Voice Rang and Place of Conversational Voice by Profoundly Hearing Impaired Person. J Head and Neck Dis. 2002;6:40.
14. Nikerson RB. Characteristics of the Speech of Deaf Persone. Volta Rev. 1975;77:342–62.
15. Higgins MB, McCleary EA, Carney AE, Schulte L. Longitudinal changes in children's speech and voice physiology after cochlear implantation. Ear Hear. 2003;24(1):48–70.
16. Giusti MC, Padovani MMP, Behlau M, Granato L. The coice of hear-ing impaired children. Braz J Otorhinolaringol. 2001;67:29–35.
17. Gilbert HR, Campbell MI. Speaking fundamental frequency in three groups of hearing-impaired individuals. J Commun Disord. 1980;13(3):195–205.
18. Monsen RB. Toward measuring how well hearing-impaired children speak. J Speech Hear Res. 1978;21(2):197–219.
19. Forner LL, Hixon TJ. Respiratory kinematics in profoundly hearing-impaired speakers. J Speech Hear Res. 1977;20(2):373–408.
20. Brown WS, Goldberg JR, Donald M. An Acoustic Study of the Intelligible offense of hearing Impaired Children Speakers. Folia Phoniatr. 1990;42:230–8.
21. Stratton WD. Intonation feedback for the deaf through a tactile display. Volta Rev. 1974;76:26–35.
22. Martony J. On the correction of the voice pitch level for severely hard of hearing subjects. Am Ann Deaf. 1968;113(2):195–202.
23. Monsen RB, Engebretson AM, Vemula NR. Some effects of deafness on the generation of voice. J Acoust Soc Am. 1979;66(6):1680–90.
24. Binnie CA, Daniloff RG, Buckingham HW, Jr. Phonetic disintegration in a five-year-old following sudden hearing loss. J Speech Hear Disord. 1982;47(2):181–9.
25. Weatherley CC, Worrall LE, Hickson LM. The effect of hearing impairment on the vocal characteristics of older people. Folia Phoniatr Logop. 1997;49(2):53–62.
26. Cerci U, Kandogan T, Olgun L, Gultekin G, Alper S. [The effect of cochlear implantation on voice development]. Kulak Burun Bogaz Ihtis Derg. 2006;16(3):112–21.
27. Girgin C. Speech Intelligibility of Turkish Hearing- Impaired Children. ISEC. Manchester. 2000..
28. Bolfan-Stosic N, Simunjak B. Effects of hearing loss on the voice in children. J Otolaryngol. 2007;36(2):120–3.
29. Hocevar-Boltezar I, Vatovec J, Gros A, Zargi M. The influence of cochlear implantation on some voice parameters. Int J Pediatr Otorhinolaryngol. 2005;69(12):1635–40.
30. Evans MK, Deliyski DD. Acoustic voice analysis of prelingually deaf adults before and after cochlear implantation. J Voice. 2007;21(6):669–82.
31. Higgins MB, McCleary EA, Ide-Helvie DL, Carney AE. Speech and voice physiology of children who are hard of hearing. Ear Hear. 2005;26(6):546–58.
32. Kent RD, Ball MJ. Voice Quality Measurement.: Singular Publishing Group; 2000.
33. Dehqan A, Scherer RC. Objective voice analysis of boys with profound hearing loss. J Voice. 2011;25 (2):e61–5.
34. Ross M, Duffy RJ, Cooker HS, Sargeant RL. Contribution of the lower audible frequencies to the recognition of emotions. Am Ann Deaf. 1973;118(1):37–42.
35. Ferrand CT. Relationship between masking levels and phonatory stability in normal-speaking women. J Voice. 2006;20(2):223–8.
36. Dehqan A, Ansari H, Bakhtiar M. Objective voice analysis of Iranian speakers with normal voices. J Voice. 2010;24(2):161–7.
37. Hall KD, Yairi E. Fundamental frequency, jitter, and shimmer in preschoolers who stutter. J Speech Hear Res. 1992;35(5):1002–8.
38. Ferrand CT. Harmonics-to-noise ratio: an index of vocal aging. J Voice. 2002;16(4):480–7.
39. Awan SN, Frenkel ML. Improvements in estimating the harmonics-to-noise ratio of the voice. J Voice. 1994;8(3):255–62.
40. Hillenbrand J. A methodological study of perturbation and additive noise in synthetically generated voice signals. J Speech Hear Res. 1987;30(4):448–61.